
In 2005 federal law compelled retailers nationwide to move pseudoephedrine, sold as Sudafed, from over the counter (OTC) to behind it to combat its use in making illicit methamphetamine. This switch prompted manufacturers to change the formulas of cough and cold medicines in the U.S. It also led my colleague Leslie Hendeles and me to prove that pseudoephedrine's replacement, oral phenylephrine, was ineffective as a decongestant.
We petitioned the U.S. Food and Drug Administration twice, but it took the agency more than a decade and a half to act on our findings. Last September an agency advisory panel finally agreed with our conclusion that this compound does little to quell congestion and recommended that products containing it be pulled from shelves. If the FDA acts on this recommendation, oral phenylephrine could be the first OTC drug approved under the agency's so-called “monograph” review process to be discontinued. But until then, millions of people who trusted the FDA and its OTC regulatory process to ensure medications work will have been wasting money on ones that don't.
FDA regulation of OTC medications with older ingredients needs to change. In the process of figuring out that oral phenylephrine isn't effective, we also spotlighted a loophole in the FDA's regulatory process that must be fixed so that people can trust not just recent OTC approvals but historic ones as well.
On supporting science journalism
If you're enjoying this article, consider supporting our award-winning journalism by subscribing. By purchasing a subscription you are helping to ensure the future of impactful stories about the discoveries and ideas shaping our world today.
Once pseudoephedrine was moved behind the counter in the 2000s, phenylephrine was the only remaining oral decongestant sold on the shelves of pharmacies, grocery stores, convenience stores, and other retail outlets. Makers of oral decongestants and cold remedies reformulated their products to contain phenylephrine—sold as Sudafed PE, among other brand names—instead of pseudoephedrine. Phenylephrine products went from few to many.
I learned that customers did not realize that these products had been reformulated. Consumers complained to their pharmacists when Sudafed PE did not work like the “old” Sudafed. Those pharmacists then contacted me at the University of Florida Drug Information and Pharmacy Resource Center, a laboratory that, among other services, teaches doctor-of-pharmacy students how to receive, research and answer drug-related questions. They asked us: Does oral phenylephrine work? If so, what is the correct dose?
My students and I searched the literature. We located an article by Hendeles published in 1993. He was reporting on well-done but unpublished studies conducted by Hylan A. Bickerman of Columbia University before 1971. Bickerman's research showed that phenylpropanolamine, a common oral decongestant at the time, worked, as did pseudoephedrine, but oral phenylephrine did not. Hendeles's paper did not get much attention, because phenylephrine wasn't widely used in the 1990s. Roughly 10 years later, however, it was suddenly important.
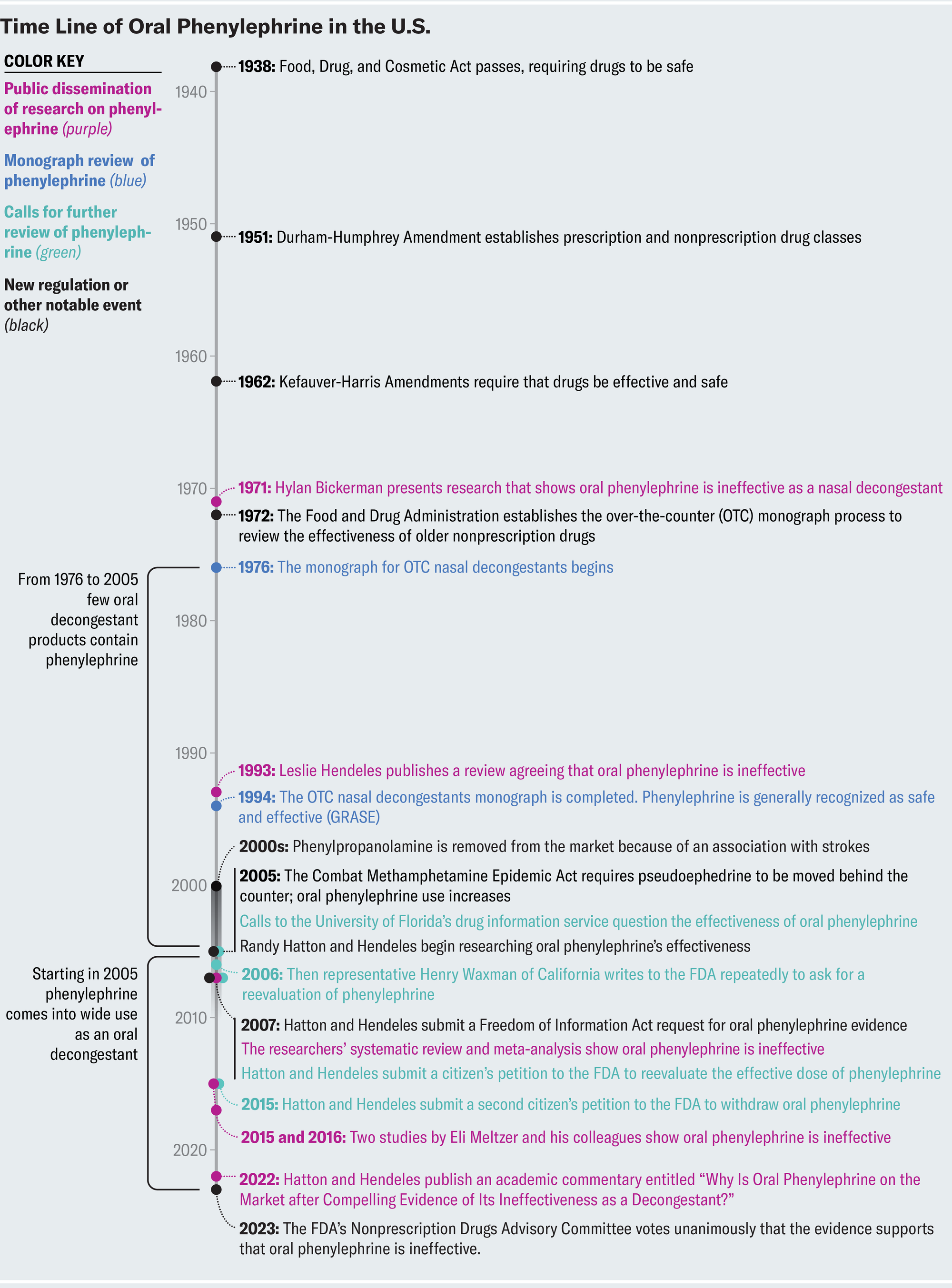
Credit: Amanda Montañez; Source: Randy Hatton (time line data)
I contacted Hendeles, who is now a professor emeritus at the University of Florida, and he and I decided to get to the bottom of oral phenylephrine's efficacy. After the FDA moved to require that drugs be shown to work, it evaluated the efficacy of OTC drugs already on the market by having expert panels review existing data on them. These OTC monographs now determine which older OTC ingredients can be marketed without FDA approval.
The monograph panel for oral decongestants reviewed a few published studies and multiple unpublished studies for phenylephrine. Of the unpublished studies, only four showed oral phenylephrine was effective, and seven showed it was no better than a placebo. We obtained copies of all the evidence used by the nasal-decongestant review panel via a Freedom of Information Act request and performed a systematic review and meta-analysis ourselves.
Our findings validated the concerns raised by the Bickerman study and the pharmacists' calls to the University of Florida. Interestingly, we found that one commercial lab gave strikingly positive results for oral phenylephrine's efficacy. The low variability of the data, a lack of increasing effect with increased dose and the lack of a placebo response prompted us to look at that report more closely. A statistical analysis of the lab's data suggested integrity issues; measurements of variables are typically expected to show uniform distribution from zero to nine for the last digit, but here nearly a quarter of all measurements ended with a five. Such anomalies occur when data are falsified. We were confident at that point that oral phenylephrine did not work.
We then naively contacted the FDA to explain what we had found. The agency was not interested—oral phenylephrine was not harming anyone, so it saw no need to limit sales. The FDA takes a risk-based approach to regulatory actions because it has limited resources, and the relative safety of oral phenylephrine relegated the drug to the back burner despite its ineffectiveness. So we went the political route, contacting then Representative Henry Waxman of California, whose committee at the time had FDA oversight. Waxman's office wrote four letters imploring the agency to reconsider oral phenylephrine's effectiveness. We also submitted a citizen's petition to the FDA in early 2007.
Finally, in December 2007, more than a year after we first discovered that oral phenylephrine didn't work, the FDA somewhat begrudgingly convened a Nonprescription Drugs Advisory Committee meeting to review the compound's effectiveness.

Credit: Joe Raedle/Getty Images
The FDA has multiple regulatory processes for different types of medicinal compounds. People are perhaps most familiar with the New Drug Application process, which requires clinical trials for prescription drug approvals. But many OTC or nonprescription drugs are regulated differently. In fact, the categories of prescription and nonprescription drugs were created in 1951 as part of the Durham-Humphrey Amendment to the 1938 Food, Drug and Cosmetic Act. In 1962 the act was amended again so that drugs had to be proved not only safe but also effective, hence the requirement for well-done clinical trials.
But what about the drugs that were approved before 1962? This window has become a loophole that some OTC drugs fall through. For prescription drugs, the FDA tried to address pre-1962 approvals through a review of more than 3,000 substances. Most of those drugs have now been reviewed and addressed, but there are still unapproved prescription medications on the market today, such as an extended-release form of oral nitroglycerin that is used to treat chest pain, among other conditions.
For nonprescription drugs, 10 years after the 1962 amendment to the Food, Drug and Cosmetic Act, the FDA established the OTC monograph process, which required products that hadn't been proved effective to be reconsidered. The FDA formed advisory panels grouping hundreds of ingredients into 26 categories based on the products' uses. After gathering all available information, both published and unpublished, from manufacturers, the advisory panels issued final reports to the FDA about whether these ingredients were GRASE (generally recognized as safe and effective), not GRASE or inconclusive. GRASE ingredients can be used in nonprescription drugs without FDA approval if the use matches the one presented in the ingredient's monograph.
The monograph for OTC nasal decongestants was started in 1976 and listed three oral drugs: phenylephrine, phenylpropanolamine and pseudoephedrine. The review took 18 years, and the final monograph was released in 1994. Phenylpropanolamine was removed from the market in the 2000s because it was associated with strokes. It was effective—just not safe.
At the time most OTC nasal decongestants contained either phenylpropanolamine or pseudoephedrine. Few contained oral phenylephrine, perhaps because manufacturers privately questioned its effectiveness. The FDA's charge for the 2007 Nonprescription Drug Advisory Committee was to determine whether phenylephrine in a 10-milligram immediate-release oral formulation can be effective when dosed every four hours for symptomatic relief of nasal congestion. Although most of the committee members voted that there was some evidence of effectiveness, they recognized the limitations of the available evidence. They asked for new data on the absorption and efficacy of oral phenylephrine obtained using more modern standards.
Schering-Plough, the maker of Claritin-D (an allergy medication that contains loratadine and pseudoephedrine), was already studying phenylephrine as an alternative oral decongestant. The company funded research on the subject, including two studies that found phenylephrine was no better than a placebo in patients with seasonal allergies who were exposed to allergens (grass and ragweed) in a controlled chamber.
The oral absorption of phenylephrine is erratic. Perhaps that's why it wasn't used as an oral decongestant until it was the only choice in front of the counter. It had long been known that enzymes in the lining of the gut metabolize oral phenylephrine into inactive metabolites, reducing the amount of the active compound that can enter the bloodstream. The most cited study on the topic found that an oral dose of phenylephrine had an absorption rate of 38 percent, but the researchers measured more than just the compound's active form. Later studies with more sensitive tests found that less than 1 percent of oral phenylephrine entered the bloodstream in an active form. Phenylephrine causes blood vessels to constrict, but if there isn't enough of the active compound in the bloodstream, it won't reduce the swelling of nasal blood vessels enough to aid in reducing nasal congestion.
After the 2007 FDA advisory committee suggested that better data on phenylephrine's efficacy were needed, Schering-Plough funded two studies led by Eli O. Meltzer of the Allergy & Asthma Medical Group & Research Center in San Diego. The work showed that oral phenylephrine was no better than a placebo—even when patients received up to four times the approved dose. In light of Meltzer's research, we filed a second citizen's petition in 2015. The science was clear: oral phenylephrine does not work. Then we waited. Nothing seemed to happen at the FDA. We wrote an academic commentary in 2022 asking, “Why Is Oral Phenylephrine on the Market after Compelling Evidence of Its Ineffectiveness as a Decongestant?” We did not know that with a new administration and new FDA commissioner, the agency had already started a thorough review of all the available data.
In 2023, 16 external experts on the second Nonprescription Drug Advisory Committee looked at all the evidence compiled by FDA staff, heard manufacturers' arguments in favor of oral phenylephrine's efficacy, and heard from experts like me who argued that oral phenylephrine is ineffective. In the end, they concluded that oral phenylephrine is not GRASE. A final ruling on whether decongestants containing the drug can still be sold will take time. We hope science will prevail.
From this experience we've learned that the monograph process for OTC drugs approved before 1962 needs to be reexamined. Systematic reviews of the available evidence indicate that other nonprescription drugs such as guaifenesin (sold in Mucinex and Robitussin), dextromethorphan (sold in Robitussin DM) and antihistamines marketed for colds (for instance, chlorpheniramine) probably don't help with coughs and colds. They are usually not dangerous, but their effects are likely to be the result of a placebo response; more modern research is needed.
The outcome for oral phenylephrine shows that the FDA needs more funding to look at old drugs. We need public funds to support independent researchers who want to examine these products objectively. The government should be able to spend millions to save consumers billions on ineffective products. Companies that market these products have no incentive to prove they don't work. Nonprescription drugs must be effective, not just safe.
If you are concerned about all the confusion around these drugs, remember that pharmacists receive considerable education on OTC drugs—more than any other health-care professionals. Ask your pharmacist when you have questions about which OTC products to choose. And then ask your local congressional representatives to support modern scientific reviews of old OTC products. We can't make guarantees about your respiratory health, but your wallet will see the rewards.
This is an opinion and analysis article, and the views expressed by the author or authors are not necessarily those of Scientific American.